
Research Foundations: MacMillan's Neurodiverse Family Systems Theory and the Science Behind Every Tool
A Framework Built on Theory, Research, and Neurological Reality
The R.E.A.L. Neurodiverse™ Framework didn't emerge from intuition alone. Every tool, assessment, and integration practice in the program is grounded in established research, peer-reviewed literature, and a coherent theoretical foundation built specifically for neurodiverse relational systems.
Step in. The structure — and the support — are already here.
Grounded in Research. Designed for Practice.

The theoretical foundation of the R.E.A.L. framework draws from multiple established fields including neurodiversity studies, empathy research, trauma-informed care, developmental psychology, and family systems theory. MacMillan's Neurodiverse Family Systems Theory and broader Neurodiverse Relational Systems Theory bring these threads together into a coherent framework designed specifically for the relational dynamics that emerge when autistic and non-autistic individuals live, love, and grow alongside one another.
The assessments, mapping tools, and integration practices throughout the program are each anchored in specific constructs drawn from peer-reviewed research: areas such as emotional interpretation, interoceptive awareness, empathy style, theory of mind, and sensory processing. These aren't borrowed loosely from adjacent fields. They are applied with care and precision to the specific realities of neurodiverse relationships.
For providers, this means you are not offering clients a proprietary system built on untested assumptions. You are offering something with intellectual depth, theoretical coherence, and a growing evidence base delivered in a format that is accessible, structured, and immediately applicable in practice.
The sections below offer a brief window into the R.E.A.L. research foundations. They aren't exhaustive; they're illustrative. Each one represents a domain of research that directly shapes how the R.E.A.L. framework understands neurodiverse relationships, and why the tools are built the way they are.
Genetic and Familial Patterns in Neurodiversity: Why the Whole Family System Matters

When a couple or family comes in struggling, it's easy to see individuals in conflict. But neurodiversity rarely arrives in isolation. Research consistently shows that neurodivergent traits cluster within families. Which means the room you're sitting in may already be a neurodiverse family system. It just hasn't been recognized as one yet.
Studies examining autism and ADHD have documented patterns of familial co-aggregation: multiple forms of neurodivergence appearing across generations within the same family. Genetic research has begun to identify possible biological mechanisms underlying these patterns, including genes such as SHANK2, which may contribute to overlapping traits across both conditions. While this research is still developing, it supports a foundational premise of the R.E.A.L. framework: neurodiversity is often a family-wide reality, not an individual diagnosis floating in a relational vacuum.
This matters clinically. When providers begin to recognize the full neurodiverse landscape of a family system, rather than treating one member's traits as the variable to be managed, the dynamics shift. Communication differences become mutual. Stress responses become understandable. And the work becomes genuinely relational.
Selected Works
Ghirardi, L., Brikell, I., Kuja-Halkola, R., Freitag, C. M., Franke, B., Asherson, P., Lichtenstein, P., & Larsson, H. (2018). The familial co-aggregation of ASD and ADHD: A register-based cohort study. Molecular Psychiatry, 23(2), 257-262, doi:10.1038/mp.2017.17.
Ma, S.-L., Chen, L. H., Lee, C.-C., Lai, K. Y. C., Hung, S.-F., Tang, C.-P., Ho, T.-P., Shea, C., Mo, F., Mak, T. S. H., Sham, P.-C., & Leung, P. W. L. (2021). Genetic overlap between attention-deficit/hyperactivity disorder and autism spectrum disorder in the SHANK2 gene. Frontiers in Neuroscience. Vol. 15,649588 doi:10.3389/fnins.2021.649588.
The Science of Empathy
Modern research shows that empathy is not a single ability, but a combination of emotional, sensory, and cognitive processes that work together to help people understand one another.
Embodied Simulation and Social Understanding
When someone reaches out and the people closest to them don't respond the way they expected, it's rarely because anyone doesn't care. It may be because their nervous systems are literally doing something different.
Research in social neuroscience suggests that humans understand others' emotions and actions through embodied simulation, a process in which the brain internally mirrors what another person is experiencing. This is closely associated with the mirror neuron system, and it helps explain how people intuitively recognize emotions and intentions in others.
But this process isn't uniform. Differences in embodied processing, which vary across neurologies, directly shape how individuals read social cues, respond to emotional moments, and experience connection. What feels like indifference to one family member may simply be a different neurological pathway to understanding.
This is why the R.E.A.L. framework doesn't treat social misattunement as a failure of caring; it treats it as a difference in wiring that everyone in the room deserves to understand.
Selected Works
Gallese, V., Keysers, C., & Rizzolatti, G. (2004). A unifying view of the basis of social cognition. Trends in Cognitive Sciences, 8(9), 396-403. doi:10.1016/j.tics.2004.07.002
Keysers, C., & Gazzola, V. (2009). Expanding the mirror: Vicarious activity for actions, emotions, and sensations. Current Opinion in Neurobiology, 19(6), 666–671. doi:10.1016/j.conb.2009.10.006
Rizzolatti, G., & Craighero, L. (2004). The mirror-neuron system. Annual Review of Neuroscience, 27, 169–192. doi:10.1146/annurev.neuro.27.070203.144230
Interoception and Emotional Awareness
A family member goes from calm to completely overwhelmed with no apparent warning. No one saw it coming, including them. This pattern, which can look like overreaction or instability to the people around it, often has a quieter explanation: the body's early signals simply weren't legible.
Interoception refers to the ability to sense internal bodily states: heartbeat, breathing patterns, muscle tension, visceral sensations. These internal signals form the bridge between what the body is experiencing and what the mind can name as a feeling. When that bridge works differently, emotional awareness doesn't disappear, but it may arrive late, incompletely, or not at all until the system is already flooded.
Interoceptive differences are particularly common among autistic individuals, and research confirms that variability in this capacity significantly influences how people identify and regulate emotions, respond to stress, and engage socially. Its relationship to alexithymia, difficulty identifying and describing one's own emotional states, means these differences often show up not just as dysregulation, but as genuine uncertainty about what one is feeling and why.
The R.E.A.L. framework's interoceptive mapping tools are built from this research, helping individuals recognize and name internal states that have often gone unacknowledged, and giving families a shared language for what each person is actually experiencing before it becomes a crisis.
Selected Works
Craig, A. D. (2009). How do you feel—now? The anterior insula and human awareness. Nature Reviews Neuroscience, 10(1), 59-70. doi:10.1038/nrn2555
Garfinkel, S. N., Seth, A. K., Barrett, A. B., Suzuki, K., & Critchley, H. D. (2016). Knowing your own heart: Distinguishing interoceptive accuracy from interoceptive awareness. Biological Psychology, 114, 65–74. doi:10.1016/j.biopsycho.2014.11.004
Seth, A. K. (2013). Interoceptive inference, emotion, and the embodied self. Trends in Cognitive Sciences, 17(11), 565–573. doi:10.1016/j.tics.2013.09.007
Emotion Differentiation and Emotional Self-Awareness
A family member is clearly upset, their body is showing it, the tension is in the room, but when asked what's wrong, the honest answer is "I don't know." Not avoidance. Not deflection. A genuine inability to identify what the feeling actually is. For families and partners trying to connect across neurological difference, this moment can become a recurring wall.
Emotion differentiation refers to the ability to identify and distinguish between emotional states, to know not just that something feels bad, but whether it's anger, grief, fear, shame, or overwhelm. Research shows that individuals vary widely in this capacity, and that it sits at the foundation of emotional regulation and constructive response to stress.
When emotion differentiation is less developed, feelings don't disappear, they arrive as undifferentiated intensity. The result can look like emotional confusion, misattribution, or responses that seem disproportionate because neither the person experiencing them nor the people around them can accurately name what's happening.
The R.E.A.L. assessments map where each person in the system sits on the spectrum of emotional granularity, not to fix it, but because understanding those differences is the prerequisite for accurate relational insight. When a family can see why the same moment lands so differently for each person in the room, something shifts.
Selected Works
Barrett, L. F., Gross, J. J., Christensen, T. C., & Benvenuto, M. (2001). Knowing what you're feeling and knowing what to do about it: Mapping the relation between emotion differentiation and emotion regulation. Cognition & Emotion, 15(6), 713-724. doi:10.1080/02699930143000239
Goleman, D. (1995). Emotional Intelligence: Why It Can Matter More Than IQ. New York, NY: Bantam Books.
Empathic Emotion and Affective Resonance
Some people feel others' emotions with immediate, sometimes overwhelming intensity. Others process the same moment quietly, cognitively, with little visible response. In neurodiverse families and partnerships, these differences in empathic style are often mistaken for indifference on one side and instability on the other, when neither is accurate.
Empathy research distinguishes between recognizing another person's emotions and the degree to which someone resonates with them emotionally, a quality sometimes called affective empathy. Research confirms that both ends of this spectrum represent neurologically valid forms of empathy. The difference is in how empathy is experienced and expressed, not whether it exists.
Where this becomes especially significant in neurodiverse systems is at the intersection of affective resonance and emotion-origin awareness: the ability to recognize where a felt emotion actually came from. When those two capacities are mismatched within a family system, the results can be genuinely confusing and painful for everyone involved. The R.E.A.L. framework maps both, giving families a way to see the dynamic clearly rather than personally.
Selected Works
Bird, G., & Viding, E. (2014). The self to other model of empathy: Providing a new framework for understanding empathy impairments in psychopathy, autism, and alexithymia. Neuroscience & Biobehavioral Reviews, 47, 520-532. doi:10.1016/j.neubiorev.2014.09.021
Decety, J., & Lamm, C. (2006). Human empathy through the lens of social neuroscience. Scientific World Journal, 6, 1146-1163. doi:10.1100/tsw.2006.221
Smith, A. (2009). The empathy imbalance hypothesis of autism: A theoretical approach to cognitive and emotional empathy in autistic development. The Psychological Record, 59, 489–510. doi:10.1007/BF03395675
Theory of Mind and Perspective-Taking
One of the most enduring, and most damaging, assumptions about autistic individuals is that they lack the ability to understand what others are thinking or feeling. The research tells a more nuanced and more useful story.
Theory of Mind refers to the ability to infer and interpret the thoughts, beliefs, intentions, and emotions of others. It is the cognitive layer of empathy: the capacity to build a working model of another person's inner world. But it doesn't operate in isolation. Research increasingly shows that Theory of Mind develops in interaction with emotional processing, how intensely we resonate with others' feelings and how accurately we track where those feelings originate, and with physical and sensory processing, including embodied simulation and interoceptive awareness.
This matters deeply in neurodiverse families and partnerships, because autistic and non-autistic individuals differ across all of these dimensions, not in ways that make one neurotype more or less capable of connection, but in ways that mean each person is working from a genuinely different foundation. When those differences go unnamed, perspective-taking gaps feel personal. When they're mapped and understood, they become navigable.
The R.E.A.L. framework integrates Theory of Mind not as a deficit to remediate, but as the cognitive dimension that sits at the top of a full empathy architecture: one that includes emotional, sensory, and physical processing alongside cognitive reasoning. Understanding the whole picture helps make relational insight possible.
Selected Works
Frith, U., & Frith, C. (2006). The neural basis of mentalizing. Neuron, 50(4), 531-534. doi:10.1016/j.neuron.2006.05.001
Gallese, V. (2007). Before and below ‘theory of mind’: Embodied simulation and the neural correlates of social cognition. Philosophical Transactions of the Royal Society B: Biological Sciences, 362(1480), 659–669. doi:10.1098/rstb.2006.2002
Want a Closer Look at the Empathy Science?
The R.E.A.L. framework is built on peer-reviewed research across social neuroscience, developmental psychology, and empathy science. If you'd like to understand the research behind each dimension of the empathy architecture, you can receive a short series of three emails that walks through the science one layer at a time.
You'll receive three emails regarding:
1. The Emotional Processing layer: Emotion-Origin Awareness (EOA) and Empathic-Emotion Intensity (EEI)
2. The Physical & Sensory Processing layer: Embodied Simulation (ES) and Interoception
3. The Cognitive Processing layer: Theory of Mind (ToM)
Each email connects the research directly to what you see in neurodiverse relational work, with references to the specific peer-reviewed literature the framework draws from.
This is a structured way to understand the science behind tools you are already exploring here.
Developmental Psychology Foundations: Erikson, Piaget, and the Spiral and Staircase Models™
The theories that have shaped our understanding of human development across the lifespan are foundational, widely accepted, and genuinely useful. They are also, without exception, built on non-autistic development.
One of the most influential comes from Erik Erikson, whose theory of psychosocial development proposes that individuals progress through a series of stages from infancy through older adulthood, each one centered on a challenge that shapes psychological growth over time. Trust. Autonomy. Identity. Intimacy. Generativity. Integrity.
These are human goals. And the path toward them looks genuinely different for autistic individuals than for non-autistic ones. Without a developmental framework that reflects that difference, autistic individuals are left navigating a map that wasn't drawn for them while the people who love them struggle to understand why the journey looks the way it does.
The R.E.A.L. Neurodiverse™ framework draws on the work Erickson and three other foundational theorists and then builds upon them:
Jean Piaget — whose concepts of assimilation and accommodation describe how people learn by integrating new information and adjusting their understanding of the world.
Diana Baumrind — whose work on responsiveness and demandingness helped clarify how developmental environments support growth.
Mihaly Csikszentmihalyi — whose concept of flow highlights the importance of balancing challenge and ability for optimal development.
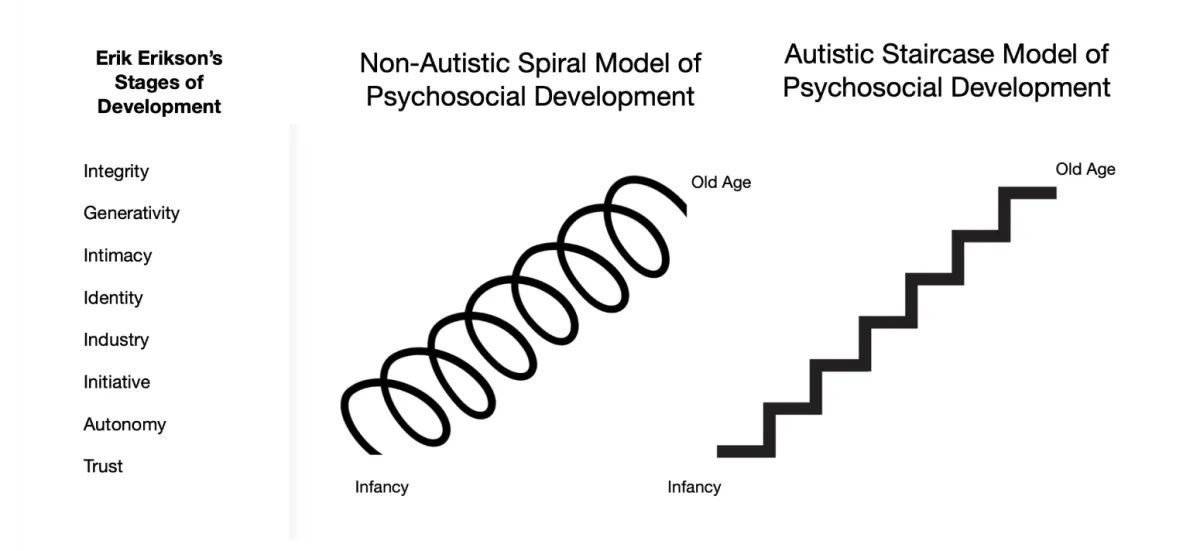
Building on these foundations, MacMillan introduces two complementary models of psychosocial development, one for each neurology, both moving upward through the same human goals:
The Spiral Model™ — representing common patterns of development among non-autistic individuals
The Staircase Model™ — representing developmental progression commonly observed among autistic individuals
Both are valid. Both lead upward. They simply take different neurological paths to get there.
These two models are not just background theory. They are the destination the R.E.A.L. framework is built toward. Every step in the 10-Step Pathway, every integration tool, every structured discussion is designed to support movement along whichever developmental path reflects each client's neurology. Step 10, the final step in the program, culminates in the Spiral Model™ for non-autistic clients and the Staircase Model™ for autistic clients, bringing the work full circle to the developmental foundation it was built on. Providers who complete the framework will find fuller descriptions of both models within the program materials.
Selected Works
Baumrind, D. (1966). Effects of authoritative parental control on child behavior. Child Development, 37(4), 887–907. doi:10.2307/1126611
Erikson, E. H. (1950). Childhood and society. W. W. Norton & Company.
Erikson, E. H. (1968). Identity: Youth and crisis. W. W. Norton & Company.
Csikszentmihalyi, M. (1990). Flow: The psychology of optimal experience. Harper & Row.
Larzelere, R. E., Morris, A. S., & Harrist, A. W. (Eds.). (2013). Authoritative parenting: Synthesizing nurturance and discipline for optimal child development. American Psychological Association.
Receive 3 Structured Emails About MacMillan's Spiral and Staircase Models of Psychosocial Development
The R.E.A.L.™ framework is built on a developmental foundation that goes beyond earlier theory: two original models of psychosocial development, one for autistic clients and one for non-autistic clients, both moving upward toward the same human goals through different neurological paths.
If you'd like to understand the theory behind the models, you can receive a short series of three emails that walks through the developmental science one layer at a time.
You'll receive:
The developmental gap: Erikson's stages of psychosocial development, how they map onto the specific psychological differences between autistic and non-autistic individuals, and what it costs clinically when that gap goes unaddressed
The Spiral and Staircase Models: MacMillan's two models of psychosocial development, grounded in the work of Piaget and Baumrind, and what each one means for how you support clients in your practice
The flow principle: Csikszentmihalyi's framework for optimal development, how it applies to both models, and how it shapes the R.E.A.L. framework's design of structure with flexibility from the ground up
Optimal Challenge and the Flow Framework
Growth doesn't happen when everything is easy. It also doesn't happen when everything is overwhelming. It happens in the space between where challenge and ability are genuinely balanced.
Psychologist Mihaly Csikszentmihalyi's research on flow demonstrated that people learn, grow, and remain engaged when the level of challenge they face is closely matched to their current abilities. Too much challenge and people shut down. Too little and they disengage. Optimal development lives in the balance.
In neurodiverse families and systems, this balance looks different for every person in the room. Differences in sensory processing, emotional integration, cognitive pacing, and communication style mean that what feels like the right level of stretch for one person may be completely inaccessible for another, or barely registering for someone else. A framework that doesn't account for this will lose people, quietly, at different points along the way.
This is the principle behind the R.E.A.L. framework's design of structure with flexibility. Providers work within a clear developmental framework while calibrating pace and depth to each individual's readiness so that growth feels possible rather than forced, and insight arrives without overwhelm.
Selected Work
Csikszentmihalyi, M. (1990). Flow: The Psychology of Optimal Experience. New York: Harper & Row.
Taken together, these research threads don't just justify the framework — they explain it. Every assessment, every integration tool, every structured discussion in the R.E.A.L. program exists because of something real that researchers have observed in how humans, and specifically neurodiverse humans, process emotion, connection, and meaning.
Providers who understand this foundation don't just use the tools with more confidence. They explain them better, hold the work more steadily, and meet their clients with greater precision.
A Program You Can Trust.
And Explain.
The R.E.A.L. Neurodiverse™ Framework is built on a foundation that holds up theoretically, clinically, and in practice. When clients ask why this approach is different, or colleagues ask what it's based on, the answer is already there. Grounded in research. Designed for neurodiverse reality. Ready to use from day one.
Grounded in research. Designed for neurodiverse reality. Ready for you.
The foundation is already built. Step in.